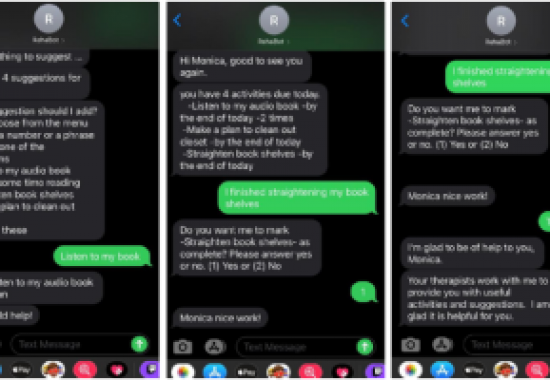
MRRI Institute Scientist Amanda Rabinowitz, PhD, was recently featured on KYW Newsradio. During her interview, Dr. Rabinowitz discussed her recent work developing a chatbot to help people with traumatic brain injury. After a brain injury, many people experience depression and loss of motivation. This can have a tremendous impact on their quality of life as well as the course of their rehabilitation. In developing the chatbot, Dr. Rabinowitz and her colleagues incorporated evidence-based principles that promote engagement and behavior change. The chatbot (called RehaBot) operates via text message and could be a key resource for patients between their therapy sessions.
“We think that this is going to be a really effective way to keep people focused on maintaining their progress and give them that sense of joy and accomplishment and pull them out of the depression,” Dr. Rabinowitz noted.
This study is one of many innovative research projects at MRRI that are incorporating rigorous, theory-driven approaches to contribute to the development of novel clinical treatments in neurorehabilitation.
Women have been integral to the evolution of MRRI from its inception, from co-founder, visionary, and scientist Myrna Schwartz, PhD, to the present day, where eleven of sixteen senior scientific staff and affiliates and two thirds of the entire Institute are women. Their positions span the spectrum of roles at MRRI, including critical daily research activities, senior leadership, administrative support, and scientist training. Our women scientists conduct theoretical, practical, prospective, and retrospective studies to advance our mission.
Having grown up in a family of progressive women in the arts and medicine and graduated from Edith Cowan University, the only Australian University named after a woman, the breadth and impact of women at MRRI is a source of pride for me. The women at MRRI make important contributions not only through brilliant thinking, efficiency, and attention to detail, but more broadly in the adaptability and interpersonal relationships that make our Institute a dynamic and collaborative environment.
During Women’s History Month and beyond, we should pause to consider the imbalance of opportunities and the challenges faced by women historically and in the present. It is important to appreciate women’s scientific, cultural, political, economic, and social achievements to date, and to recognize those who are presently blazing trails for future women.
While gender equality is improving, we should all be attentive to ensuring that women receive the opportunities in science that are experienced by men. This includes outcomes in grant and manuscript submissions that are equivalent across gender, and equal proportions of women invited as conference speakers, prestigious scientific board members, and leaders in professional organizations. I encourage you to visit mrri.org/who-we-are to learn more about the history, current innovations, and significant scientific progress being made by the women at our Institute.
The critical need for options to deliver healthcare treatments remotely has been brought into the spotlight during the COVID-19 pandemic. COVID-19 has placed limitations and restrictions on the delivery of healthcare, making traditional in-person office visits more of a challenge. Even prior to the pandemic, brain injury rehabilitation providers had noted that transportation and financial barriers limit access to in-person treatment.
MossRehab has partnered with the Brain Injury Association of Pennsylvania (BIAPA) and other local rehabilitation providers to conduct a pilot demonstration study of remote delivery of cognitive rehabilitation for persons with traumatic brain injury (TBI), funded by the Pennsylvania Department of Health. Telehealth solutions for cognitive rehabilitation (telerehab) may be more effective and efficient than in-person services alone. The ability to deliver treatment to individuals in their homes could reduce missed appointments, while increasing access to services and allowing therapists to work with patients in their home environments.
After a moderate to severe TBI, many people have difficulties with everyday thinking skills. Cognitive Rehabilitation therapy is a broad term describing treatments that address these issues. Therapists must take into account each patients’ unique situation—their cognitive strengths and difficulties, the demands of their every-day lives, and the resources and supports available to them in their home environments. Given the wide range of problems and needs of individuals with brain injury, therapy varies from person to person. Although cognitive rehabilitation may include elements that target restoration of cognitive skills, for patients with brain injury, treatments that focus on compensating for cognitive deficits have a greater positive impact on real world functioning. Compensatory therapies focus on training strategies to overcome specific problem areas, often using external aides like smart phone applications, memory notebooks, and family calendars.
There are a number of challenges to providing cognitive rehabilitation via telehealth. Not all patients have access to high-speed internet and adequate hardware, that is, a computer or tablet with video capability. In the pilot demonstration project, a program evaluation team is tracking what patients already have access to and providing hardware and internet to those who need it. They are also providing staff and patients with an initial training session and ongoing technical support. Estimating the time and effort required for training and support will be important for evaluating the feasibility and sustainability of offering telerehab services beyond the scope of the current program.
This demonstration study is enrolling patients who are receiving cognitive rehabilitation and brain injury counseling supported by the Pennsylvania Department of Health’s Head Injury Program (HIP). Just as they do in usual practice, therapists work with individual patients to develop treatment plans around their goals. For the duration of their participation, patients are provided with iPads and high-speed internet to take part in HIPPA-compliant video conferencing. Patients enrolled in the program participate for at least six months, and as long as the remaining duration of their HIP-supported benefit for cognitive rehabilitation and brain injury counseling.
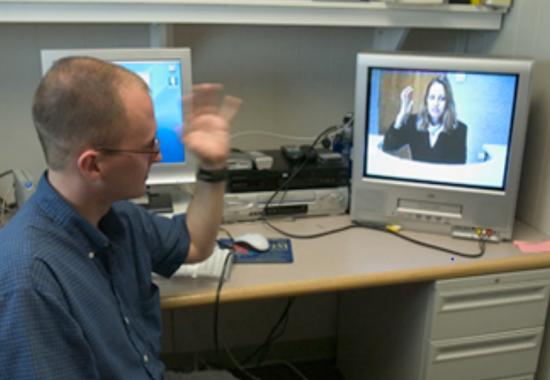
The therapists participating in the program have been holding video conference sessions with patients since March of 2020 and have noted many benefits of telerehab. Amanda Johnson is a therapist at MossRehab’s Drucker Brain Injury Center at Elkins Park. She described how video conferencing has allowed her to help patients improve their organization skills within their home environments, adding that some patients are more comfortable with video conferencing than home visits. Being able to view the patient’s home environment unlocks new opportunities for treatment. For example, Ms. Johnson was able to see the ingredients and kitchen equipment in a patient’s kitchen, which was useful in coaching them through meal planning and preparation. An added benefit that Ms. Johnson has noticed is that patients’ experiences with the iPad and video conferencing software have helped some become more comfortable with technology.
Amanda Rabinowitz, PhD, institute scientist at Moss Rehabilitation Research Institute (MRRI) and director of the Brain Injury Neuropsychology Laboratory, is leading the program evaluation team, which will evaluate feasibility and user-satisfaction with services delivered over the telehealth platform. The team is looking at several different factors related to how practical and desirable telerehab may be for patients with brain injury. One of these factors is the financial cost and technological support needed to get patients set up to use the video conferencing. Treatment providers are monitoring attendance at appointments throughout the duration of treatment, keeping track of any barriers to treatment encountered along the way. At the conclusion of the study, both patients and therapists will report on the usability of the video conference platform and their satisfaction with the experience. Both patients and providers are surveyed on the potential benefits and any potential disadvantages of holding cognitive rehabilitation visits remotely through video conference.
Eliminating the logistical challenges of transportation to and from the clinic could improve attendance. The team is interested in learning whether telerehab sessions are better attended and more easily rescheduled than in-person sessions. The team will also be investigating how clinicians make use of the opportunity to provide therapy for patients within their home environment. Do therapists involve family members, calendars, and other elements of the home environment to do real-time strategy development, for example, for the management of mail or the payment of bills?
Researchers and clinicians involved in this demonstration study were pleased to discover that patients were highly interested in participating. The team closed enrollment in January 2021 with 28 active participants, and this was considerably more than their target enrollment of 20 participants. The study will conclude at the end of May 2021, and we look forward to using these results to help us continue to develop new and innovative treatments at MossRehab.
Rehabilitation scientists and care providers have come to understand that traumatic brain injury (TBI) is a dynamic condition that often leads to health issues persisting for many years after the event. For a subset of those living with TBI, decline occurs over time and is likely due to a myriad of causes including progressive neurodegenerative processes, comorbid conditions, aging, behavioral choices, and psychosocial factors. Deterioration, whether directly or indirectly associated with the original brain injury, must be proactively managed to maximize health, independent function, and participation in society.
Moss Rehabilitation Research Institute (MRRI) Institute Scientist Amanda Rabinowitz, PhD, and Drucker Brain Injury Center Clinical Director Tom Watanabe, MD, are part of a group of researchers led by Flora Hammond, MD, of Indiana University that are working to address this need by developing a comprehensive model for the proactive management of TBI. A chronic disease approach to TBI would include identification of risk and protective factors, protocols for early identification, evidence-based preventive and ameliorative treatment, as well as development of self-management training approaches. The project will take 5 years to complete, and it is supported by funding from the National Institute of Disability, Independent Living, and Rehabilitation Research (NIDILRR).
Management of chronic diseases, such as diabetes and heart disease, differs from medical management of acute conditions. Care of individuals with chronic conditions must be coordinated across primary and specialty care providers. Patients themselves must take an active role in day-to-day decisions about the management of their illness. Effective chronic care management relies on the partnership between patients and health care professionals. When patients are more informed, involved, and empowered, they interact more effectively with the healthcare system and make lifestyle choices to promote better health.
Drs. Hammond, Watanabe, Rabinowitz, and their colleagues want to extend this chronic disease approach to people living with TBI. The model they are developing is called “BeHEALTHY,” and it aims to transform treatment of chronic TBI by optimizing diagnosis, evaluation, and management of patients with TBI. This approach is designed as a cooperative model, encompassing primary and specialty care providers, patients, and their caregivers, as well as modifications to the health care system.
This comprehensive approach will involve broad efforts spanning professional education, development of tailored self-management approaches, and structural changes to healthcare systems. For example, clinicians who are not brain injury specialists will require training in methods for identifying TBI in their patients, as well as education on common medical comorbidities and best practices for treating these conditions in the context of TBI. To develop tailored self-management approaches for improving physical and mental health in people with TBI and their caregivers special attention must be given to common cognitive and physical limitations of TBI. These self-management programs may include community resources and peer support groups, as well mobile apps to assist with self-monitoring. In order to ensure that clinical and self-management programs are feasible and sustainable, the group will also design modifications to the health care system to support these efforts. For example, changes to the medical record and billing/funding practices would facilitate communication across care providers and ensure broad access to care. In developing this comprehensive approach, the team is drawing from models of care shown to be effective for other chronic conditions.
Since the project began at the end of last year, the research team has been reviewing the medical literature to inform the development of the BeHEALTHY model. Once developed, the model will be refined using input from people living with brain injury and their caregivers. Over the final two years of the project, the research team will conduct clinical trials to test the components of BeHEALTHY for feasibility, and they will begin disseminating the program to healthcare systems across the country. “The goal is to transform care, so that people with TBI can live longer, healthier, happier, and more productive lives,” notes Dr. Rabinowitz. MossRehab is proud to be one of the TBI Model Systems sites that is participating in this important project. Dr. Watanabe lends his expertise on clinical management as part of the work group that is developing guidelines for clinical care. Dr. Rabinowitz is overseeing all project-related research activities at Moss and contributing to the effort to develop self-management approaches.
Umi Venkatesan, PhD, who directs the Brain Trauma and Behavior (BraTBehavior) Laboratory, recently launched a project examining social factors that may affect the recovery of adults with traumatic brain injury (TBI). This exciting work is funded by the Albert Einstein Society, and it focuses on pre-injury, early life experiences that may shape how individuals recover from TBI sustained in adulthood.
Why do pre-injury experiences matter? Oftentimes what we think of as “brain injury outcomes” are in fact much more than that. When we ask someone how they are doing emotionally or about their social relationships, we are not just capturing their life now (since their injury) but the effects of all their life experiences (before and after injury) combined. For example, it is well documented that TBI can negatively affect mental health, but a person’s emotional functioning is also influenced by whether they may have struggled with psychological problems in the past. As one might expect, problems present before injury do not stop being relevant after injury; in fact, they are at risk of worsening. In other words, TBI changes someone’s life, but it does not erase who they were before their brain injury.
Previous research has centered mostly on demographic factors that influence TBI outcomes, such as sex, race, and socioeconomic status, but these do not tell us much about a person’s “lived experience” before injury. We know that social experiences earlier in life can have significant impacts on how people approach daily life activities and, importantly, how they cope with stress. Indeed, recovering from TBI can be a major source of stress!
In his current work, Dr. Venkatesan is asking survivors of TBI about negative childhood family and social experiences that may ultimately affect how well they recover from TBI. In the general population, these experiences have been shown to have a number of negative health effects later in life, including increasing the risk for sustaining a TBI. Dr. Venkatesan’s lab is examining whether these kinds of experiences may have similar effects on outcomes after TBI. The long-range goal is to bring us closer to a more holistic understanding of each patient, which would allow clinicians to better personalize treatment to reflect the life perspectives of each individual. Dr. Venkatesan argues that while demographic factors and the effects of injury on the brain are not easily changed, we can better understand and modify attitudes and behaviors that could interfere with recovery potential. This approach may prove fruitful in improving the quality of life of those impacted by TBI.
Recruitment for this study is underway, and several participants have already been enrolled. The project will run through 2021, and Dr. Venkatesan expects to collect data on 80-90 individuals living with TBI in the Philadelphia region. The study is believed to be the first of its kind, and it has already led to collaborations with other TBI investigators across the country. With these scientists, Dr. Venkatesan recently founded a research workgroup devoted to characterizing pre-injury functioning in individuals with TBI. This initiative, known as Lives Before Brain Injury (LiBBI), meets monthly to discuss methodological and conceptual issues, share current research projects of its members, and identify collaborative opportunities.
Dr. Venkatesan’s research program at MRRI hopes to address a critical gap in the literature regarding individual life trajectories and how they may be modified by TBI. The BraTBehavior Laboratory is fortunate to be able to conduct this work within the diverse population of the Delaware Valley and looks forward to expanding its scientific mission with future research partnerships.
This week, Moss Rehabilitation Research Institute (MRRI) published the 2021 edition of our annual newsletter, MRRI Letters.
In this edition, we include a message from MRRI Director Dylan Edwards, PhD; a story from a research participant about participating in research at MRRI; recent successes and accomplishments; interviews with two recent postdoctoral fellows on their training experiences at MRRI, and highlights from each of our research focus areas.
You can learn more about the innovative projects our scientists have been working on related to imitation and tool use in limb apraxia, assessing navigation difficulties after stroke, animal-assisted therapy for aphasia rehabilitation, and the neuropsychology of traumatic brain injury.
Catch up on the news and updates from our scientists and research laboratories from 2021 with MRRI Letters.
Since founded in 1992, Moss Rehabilitation Research Institute has maintained a leading role in the study of Traumatic Brain Injury (TBI). In honor of Brain Injury Awareness month, we are highlighting some new and ongoing projects to advance the understanding and treatment of TBI. To kick off the month, let’s first look at some of the key contributions to brain injury rehabilitation research throughout the institute’s history.
The TBI Model System
Since 1997, MossRehab has retained its status as a TBI Model System. The National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) provides funding for institutions recognized as national leaders in clinical research and patient care through its TBI Model Systems grant program. A Model System is a center of excellence that performs at the highest level in research and treatment of a particular condition.
MossRehab has received funding as a TBI Model System Center since 1997. Over more than 20 years, MRRI Scientists and MossRehab clinicians have led and contributed to state-of-the-art research studies, shared their findings with the public, and provided comprehensive clinical care to help guide patients from traumatic brain injuries through re-entry into community living.
The Moss Traumatic Brain Injury Model System led by MRRI Institute Scientists Amanda Rabinowitz, PhD, and John Whyte, MD, PhD, is one of only 16 TBI Model Systems in the United States and the only Model System in Pennsylvania. MRRI scientists collaborate with clinicians at the Drucker Brain Injury Center at MossRehab Elkins Park to conduct cutting-edge research on brain injury while providing world-class patient care for those with brain injury.
John Whyte’s Pioneering Work on the Rehabilitation of Patients with Disorders of Consciousness
Dr. Whyte’s research has focused on assessment and treatment of patients with traumatic brain injury, including those with disorders of consciousness. Throughout his career, he has participated in the key research, policy, and ethical developments addressing this patient population.
Dr. Whyte received the American Congress of Rehabilitation Medicine’s Lifetime Achievement Golden Key Award in recognition of his work. Read more about his research, including his work on disorders of consciousness.
Tessa Hart’s Distinguished Work on Cognition and Emotional Functioning after TBI
Tessa Hart, PhD, is a scientist emerita at MRRI, with a program of TBI research spanning more than 20 years. A major focus of her research is creating and testing interventions to improve executive function and emotional status using theoretically-based, self-regulation models.
Dr. Hart received The Robert L. Moody Prize for Distinguished Initiatives in Brain Injury Research and Rehabilitation in 2019 in recognition of her work:
Recently, Dr. Hart led a study to evaluate the impact of a new protocol for caring for patients with severe memory deficits (called post-traumatic amnesia) due to acute TBI. Learn more about the post-traumatic amnesia (PTA) protocol developed by Moss scientists and clinicians.
The Development of Novel measures to Assess Brain Injury Outcomes
MRRI scientists have led the development of tools for assessing individuals with traumatic brain injury.
The Moss Attention Rating Scale (MARS) was designed as an observational rating scale to provide a reliable, quantitative and ecologically valid measure of attention-related behavior after TBI. Learn more information about the MARS tool.
The Brain Injury Functional Outcome Scale (BI-FOM) provides a measure of global functioning after moderate-severe TBI. It was designed to capture variations in function among individuals at both high and low levels of impairment. Read about BI-FOM.
The Brain Injury Nociception Assessment Measure (BINAM) is a measure of nociception designed to assess pain, independent of the level of consciousness. . Assessing painful conditions in Individuals with impaired consciousness after severe brain injury previously was a challenge. Read about BINAM.
The Development of Novel Treatments
MRRI Scientists are at the forefront of developing and testing pharmacologic and behavioral interventions for individuals with TBI.
Dr. Whyte co-led (with Joseph Giacino of Spaulding Rehabilitation Hospital) a randomized placebo-controlled trial of amantadine, which demonstrated, for the first time, that a treatment could accelerate the pace of recovery of consciousness. The amantadine trial was published in the New England Journal of Medicine (2012) and led to large scale adoption of this treatment. Read about the successful trial of amantadine for accelerating the recovery of consciousness after very severe brain injury.
In 2011, Dr. Hart, colleagues from MRRI and Craig Hospital in Englewood, Colorado launched the first multicenter, randomized-controlled trial of a psycho-educational treatment for anger following TBI. The anger self-management training was effective and showed durable benefits for reducing some aspects of problematic anger. Results in the Journal of Head Trauma Rehabilitation (2017). Read about Regulating Emotion After Traumatic Brain Injury.
In 2019, Dr. Hart published the results of a randomized-controlled trial evaluating a treatment for depression and/or anxiety in individuals with moderate to severe TBI. The treatment in this study is based on Behavioral Activation (BA)—an intervention that focuses on increasing involvement in rewarding and pleasurable activities. Those in the BA condition reported more exposure to environmental reward and greater productivity. Read about Promoting Health After TBI.
TBI Scientists join the MRRI team
In recent years, the TBI research program at MRRI has added two new laboratories.
In 2015, Dr. Rabinowitz, came to MRRI to direct the Brain Injury Neuropsychology Laboratory. With research focused on cognitive and emotional sequelae TBI, she brings expertise in mild TBI and sports-related concussion to the TBI research team.
In 2019, Umesh Venkatesan, PhD, joined the TBI research team, bringing his expertise in neuroimaging and assessment of memory and social cognition in the context of TBI. He established the Brain Trauma and Behavior Laboratory (BraTBehavior), which studies aging with TBI and proposed links between chronic TBI and neurodegeneration.
MRRI scientists have contributed substantially over the years to advancing our understanding of traumatic brain injury and developing novel assessment and treatment methods. We look forward to conducting more innovative research in this area with the goal of improving the lives of individuals with neurological disabilities through research.
Moss Rehabilitation Research Institute (MRRI) Founding Director and Institute Scientist Emeritus John Whyte, MD, PhD recently discussed his career, research, and life outside of science on the People Behind the Science podcast hosted by Marie McNeely, PhD.
During the interview, we learn about Dr. Whyte’s interests beyond research and medicine, including his passion for music. He also describes some of the key mentors and important steps along his career that led him in helping to create MRRI.
January was a busy and productive month for MRRI scientists and staff as we continue to remotely foster connections and collaborations with neurorehabilitation experts from other leading institutions to further advance neurorehabilitation research.
As part of the MossRehab Shrier Family Topics in Rehabilitation Science Lecture Series, MRRI welcomed back a former MRRI postdoctoral fellow, Denise Harvey, PhD as a visiting speaker. A Research Associate Professor in the Department of Neurology at the University of Pennsylvania, Dr. Harvey presented her work on using noninvasive brain stimulation to enhance recovery in people with aphasia.
Brenda Rapp, PhD, also joined us virtually to present in MRRI’s Institute Forum. Dr. Rapp is working to better understand language recovery after stroke or other brain injury. She serves as a Professor in the Department of Cognitive Science at Johns Hopkins University.
New Research Collaborations
Amanda Rabinowitz, PhD, will collaborate with investigators from the Rehabilitation Hospital of Indiana in Indianapolis on a project funded by the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR). Dr. Rabinowitz will serve as a site principal investigator on a multi-site study led by Flora Hammond, MD to examine chronic disease management in people with traumatic brain injury (TBI). This project will leverage resources of the MossRehab TBI Model System as well as TBI Model Systems across the country. By producing new knowledge to address evidence gaps in the management of brain injury as a chronic condition, the research team looks to reduce mortality and improve health, function and quality of life for people with TBIs.
Dylan Edwards, PhD, will work alongside Hermano Igo Krebs, PhD, from MIT as co-chair of a Special Interest Group on Rehabilitation Robotics for the World Federation for Neurorehabilitation (WFNR). In this role, Dr. Edwards will further the development of rehabilitation robotics through meetings and educational activities during the WFNR World Congress and beyond.
We are proud to announce that Gabriella Vigliocco, PhD, was recently named among the 2021 Fellows of the Cognitive Science Society, a global professional organization that connects scientists from diverse research fields to advance our understanding of the human mind. Fellows are elected yearly based on the sustained excellence and impact of their research on the Cognitive Science community.
Founded in 1979, the Cognitive Science Society has selected fewer than 200 scientists to be honored as Fellows. Dr. Vigliocco now holds this prestigious distinction among renowned researchers, including Alfonso Caramazza, Noam Chomsky, Steven Pinker, Susan Carey, and Michael Posner.
A Professor of the Psychology of Language at that University College London and a Scientist in Residence at MossRehab Research Institute (MRRI) since 2017, Dr. Vigliocco discusses her research and this exciting honor.
Q: What were your initial thoughts when first receiving the news about becoming a Cognitive Science Society Fellow?
I was really excited, it is a great honor! And it is always incredibly nice that someone among your peers nominated you without knowing it. It is an important reminder that we should find time to promote the work of others.
Q: Is there a particular Fellow who you particularly respect or have considered a role model?
There are many on that list that I’ve considered as role models: Larry Barsalou, Kay Bock, Gary Dell, Pim Levelt, Jay McClelland, Susan Goldin-Meadow, and Barbara Twersky.
Q: Can you describe some of your works’ key findings and their impacts on the cognitive science community?
I’d like to think that I’ve contributed to and led a shift in the fields of psychology, neuroscience, and linguistics from studying language as a symbolic capacity that was evolved, learned, and used separately from the rest of human cognition, to one in which language is grounded in basic sensorimotor functions that should be studied in its ecological niche.
Our work on abstract concepts is one example of precisely moving our thinking of language and conceptual knowledge from purely symbolic to grounded. My group provided the first evidence that abstract words and concepts (e.g., idea) are rooted in the neural system processing emotions rather than high-level symbolic operations. Thus, we brought attention to emotional experience as key in providing grounding to concepts (going beyond a sensory-motor view of embodiment). This finding resulted serendipitously while re-assessing the difference between concrete and abstract word processing. It was a genuinely new discovery and took us some time to convince the cognitive science community. Our finding has important implications for development. We have demonstrated that younger children are better able to learn abstract words that have emotional connotations.
Our current work investigates language learning and processing in its ecological niche ( face-to-face communication). Language is usually defined as speech or text, ignoring the multimodal cues that accompany speech in face-to-face communication. This is despite the fact that the brain learns and processes language mostly in face-to-face contexts. In our current work, we focus on the multimodal cues (points, gestures, object manipulations, eye gaze) in learning new words and concepts and in processing language. In collaboration with MRRI scientist Laurel Buxbaum, PsyD, we have identified the brain networks engaged in coordinating and integrating speech with gestures for the first time. This is the first step in characterizing the neural substrate of multimodal language.
Q: How have collaborations shaped your research?
Collaborations make my research possible. First, I am a social researcher, meaning that I develop my best ideas by talking to others. Second, I am an interdisciplinary researcher. I fully believe that to tackle the broader, more interesting, and pressing questions, we need to go outside our silos and work across disciplines at different analysis levels. As such, I can only conduct my research in collaboration with others. I have been extremely fortunate to have always encountered excellent collaborators across the years, including talented scientists at MRRI. In addition to making my research possible, these collaborations have enormously enriched my personal life.
Q: What do you think junior researchers should be doing now to become leaders in their field?
Being a junior researcher is far more difficult nowadays than it was twenty or thirty years ago. The competition is so much harsher, and there is constant pressure toward publishing and obtaining grant funding. My advice would be not to focus exclusively on research topics that are mainstream, fashionable, or “hot” at the moment. Instead, dare to venture into uncharted territories and exploring less trodden paths, especially those at boundaries between different disciplines.