Understanding the impairments in motor function that humans with neurological damage experience following a brain injury or spinal cord injury could give scientists insight into opportunities to improve conventional rehabilitation treatment options and help develop more informed rehabilitation treatment strategies.
At the Human Motor Recovery Laboratory, researchers use contemporary techniques including non-invasive brain stimulation, neuroimaging, kinematics, and virtual reality, along with conventional rehabilitation therapies, to study and promote the motor recovery process.
Led by Director of MRRI Dylan Edwards, PhD, the laboratory is dedicated to finding the right combination of approaches to optimize the motor recovery process, while making it a more engaging and enjoyable experience for patients.
In this video, Dr. Edwards describes the different motor function restoration strategies used at the Human Motor Recovery Laboratory in its mission to make a difference in patients’ lives.
Rehabilitation week calls attention to the field of rehabilitation – a field that touches many lives yet is unfamiliar to many until it does. All branches of medicine seek to restore health, but rehabilitation seeks to restore function – that is, the ability to care for oneself, move about, interact with others, and more generally accomplish the life tasks that matter to us. For sudden acute illnesses, like a bout of gastroenteritis, one will likely return to normal function after recovery from the illness.
In contrast, many injuries and chronic illnesses unfortunately don’t result in full recovery (e.g., spinal cord injury, congestive heart failure), and others (e.g., lumbar disk herniation) may resolve physically but leave a person still unable to work or complete their daily activities.
Rehabilitation seeks to maximize function using a much broader set of tools than those that treat or cure the disease. Perhaps most familiar are the physical devices of rehabilitation: wheelchairs and computerized communication devices that let individuals with paralysis or speech problems function by other means. However, rehabilitation has something to offer virtually any condition that results in functional limitation.
Further, the field of rehabilitation can best serve patients by bringing together people with diverse backgrounds and skills to develop innovative treatments and deliver comprehensive care. Moss Rehabilitation Research Institute (MRRI) and MossRehab are home to scientists and clinicians with expertise spanning clinical psychology, neuropsychology, cognitive neuroscience, physiatry, occupational therapy, physical therapy, speech-language pathology, and other disciplines.
Our diverse team and cross-disciplinary approach to rehabilitation research allow us to make important contributions to the field to improve the lives of individuals with neurological disabilities. Below we introduce some of the dedicated individuals involved in rehabilitation research here, and the important roles they play in this large and varied enterprise.
My doctoral training focused on clinical psychology and neuropsychology, so I’ve always been attuned to clinical populations. A particular interest was understanding the underlying causes of the types of unusual behavior explored by neurologist Oliver Sacks, who wrote, “The Man Who Mistook His Wife for a Hat”—that is, patients in whom a specific cognitive or sensory-motor ability is affected by neurological damage, often leaving other abilities remarkably intact. An example is a disorder called limb apraxia, in which individuals with stroke or neurodegenerative disorders have lost the ability to use tools or imitate actions, despite their ability to describe the purpose of the tools, where they are found, and who might use them, despite adequate motor and sensory abilities.
Apraxia is a fine example of a complex disorder whose understanding is enriched by collaboration between researchers from multiple disciplines of scientific study, as well as clinicians: experts in motor control and arm function, language and aphasia, executive function, and memory all contribute different kinds of insights to our understanding.
Moreover, different methods of study, including neuroimaging and behavioral studies with both healthy and clinical populations have proven invaluable. This collaborative work in the Cognition and Action Lab at MRRI has yielded numerous advances in our understanding of how different brain structures contribute to distinct aspects of tool use and imitation tasks, and exactly how these processes may be disrupted by neurological disorders.
When we understand the underlying causes of dysfunction, we are better equipped to design interventions that directly target these deficits to facilitate optimal functioning.
Mary Ferraro, PhD, OTR/L
I have worked at MossRehab and the MRRI for over 35 years. Starting as a staff occupational therapist on the inpatient brain injury unit, I was able to take advantage of a research institute that valued working alongside clinicians. This opportunity caused me to examine patient performance and my practice in a more systematic way, leading to numerous research and clinical projects.
One of my current clinical responsibilities includes occupational therapy (OT) staff development, best exemplified by serving as coordinator for the MossRehab OT Fellowship Program in Physical Rehabilitation, an advanced therapy practice training program.
I have other education-related responsibilities for the brain injury center staff and the Moss Traumatic Brain Injury (TBI) Model System. Beyond the continual demand to orient new staff to the needs of individuals with brain injury, my education role seeks to improve day-to-day clinical processes using evidence to inform practice.
Over the past 18 months, Amanda Rabinowitz, PhD, and I have coordinated a knowledge translation project for patients with post-traumatic amnesia, recently published in Brain Injury. The success of the project, changing therapist questions during these patient interactions, hinged on understanding clinic routines, and creating best practices that were workable for all. I saw my role as bringing clinicians and researchers together to improve patient care.
Various research projects over the years enhanced my understanding of rehabilitation’s multidisciplinary scope. By participating in projects on naturalistic action analysis, classification of hemispatial neglect subtypes, and rehabilitation treatment specification, I have had the privilege to work alongside clinicians and researchers who want to understand rehabilitation needs better so that treatments can be enhanced.
I’m trained as a physiatrist (a physician specializing in Physical Medicine and Rehabilitation) as well as in Cognitive Psychology. I spent the first 10 years of my career working half-time clinically caring for inpatients with severe traumatic brain injury and the other half engaged in research on the cognitive impairments that result from TBI.
Since the beginning of my career, I’ve been interested in the most severe brain injuries – the ones that result in prolonged or even permanent disorders of consciousness (DOC). When I began my career, such patients were systematically excluded from rehabilitation on the premise that their prognosis was hopeless and that they could not actively participate in rehabilitation.
Nevertheless, with some early grant funding, we established a demonstration treatment program, the Responsiveness Program, and showed that rigorous analytic methods could accurately establish a patient’s state of consciousness and track recovery.
Over the years as my research portfolio grew and I was asked to lead MRRI, my responsibilities shifted to focus fully on research, but my research agenda continued to be strongly shaped by my clinical experience and my interactions with clinical colleagues, patients, and families. I’m happy to say that, through my research and studies conducted by a number of collaborators, much has changed for individuals with DOC.
We now have accurate diagnostic tools, improved prognostic abilities, evidence that a substantial minority will have good long-term outcomes, and, most recently, treatments that can accelerate the recovery of consciousness. This has culminated in the publication of a new practice guideline related to DOC that, for the first time, advocates for intensive rehabilitation for this population, based on the evidence developed over the last couple of decades, and a renewed interest at NIH in studying recovery from coma.
I am a clinical researcher and speech-language pathologist, and I have recently begun my fourth year as the director of the MossRehab Aphasia Center. The Center was founded by Myrna Schwartz and Ruth Fink in 1996 to meet the long-term rehabilitation and social needs of those living with aphasia, an acquired language impairment most typically occurring as the result of a stroke.
The guiding principle of the Center is the Life Participation Approach to Aphasia, a goal of which is to collaborate with people with aphasia and their loved ones to help them meet their unique goals for themselves. Two of our recent projects highlight these collaborations.
Our longitudinal research study, a collaboration with new members of our conversation groups, is directed toward quantifying outcomes of participation in our aphasia activities center across the domains of linguistic impairment, functional communication, and quality of life.
Our newest aphasia center program is the Persons with Aphasia Training Dogs Program. The ‘nuts and bolts’ of the program are that people with aphasia learn positive reinforcement techniques to train dogs, either their own dog or a local shelter dog, in basic obedience skills (for example ‘sit’, ‘stay’).
The goals of the program are to harness what people with aphasia can do, rather than focusing on what is difficult for them, to capitalize on the physical and psychosocial benefits of human-animal interaction, and to combat social isolation by increasing feelings of confidence and self-efficacy through new skill learning.
I look forward to the prospect of continuing to work directly with and for people with aphasia in these, and other, projects to expand the impact of our Center beyond its physical boundaries, by incorporating our programs with the local community and by contributing to the evidence base demonstrating the impact that can be made Aphasia Centers founded on the life participation approach.
I started my career as a physical therapist and gained clinical expertise in neurologic physical therapy. My clinical experience shaped three important notions:
Rehabilitation greatly enhances patients’ quality of life
The brain has an incredible capacity to change with interventions
Despite rehabilitation efforts, different patients respond differently to interventions.
My research is inspired by my clinical experience and is strongly informed by my PhD in Biokinesiology, and post-doctoral training in neuroplasticity and motor control and learning.
My research in the Neuroplasticity and Motor Behavior Laboratory investigates behavioral and neurophysiologic factors that influence the performance and learning of motor skills in individuals with and without neurologic disorders. The overarching goal is to identify cognitive-motor processes and underlying neural substrates that implement control and learning of motor skills in order to optimize rehabilitation strategies.
One line of research in our laboratory investigates behavioral, neuroanatomic, and neurophysiologic correlates of deficits in the ability to coordinate two hands after stroke. The ability to coordinate two hands is critical for most activities of daily living but often overlooked in rehabilitation research and practice. Through our research, we help identify patients who have significant deficits in bimanual coordination, and we use targeted interventions to remediate those deficits.
The second line of research in our laboratory investigates optimal behavioral and noninvasive brain stimulation interventions that lead to faster and/or better motor recovery of arm function after stroke. Recovery of arm function relies on the ability of the brain to change with practice and repetition, often referred to as neuroplasticity. While modulating neuroplasticity may influence motor recovery globally, we recognize that one size does not fit all in stroke rehabilitation. So our focus is to identify behavioral and neurophysiologic markers of learning to help guide treatment protocols to be more individualized and effective.
Like all fields of healthcare, advances in rehabilitation care are dependent on research. Clinical rehabilitation is often a team sport, reflecting the fact that human function is a complex affair involving the interaction of the body’s physical structure, movement abilities, and cognitive processes.
Accordingly, members of many different disciplines have insights to contribute. The same goes for rehabilitation research: linking simple models of thought and movement to complex functional abilities, like making a meal or navigating the environment, requires the expertise of many kinds of scientists.
We’ve introduced you to just a few of the people involved in this exciting enterprise. We are fortunate at MossRehab and MRRI to have a wide array of skilled clinicians and scientists from many disciplines, and a supportive environment that encourages cross-talk and collaboration.
A team of researchers at MRRI and clinicians at MossRehab recently came together to address an important clinical issue—how to best care for patients with severe memory deficits due to acute traumatic brain injury (TBI). With the support of the Moss Traumatic Brain Injury Model Systems, Dr. Amanda Rabinowitz and Dr. Mary Ferraro led a workgroup to develop an evidence-based protocol for treatment. The workgroup included supervisors from each of the major rehabilitation disciplines – Elizabeth Marcy (Physical Therapy), Stephanie Farm (Occupational Therapy), Deb Presutti (Speech Therapy), Nicole Bongart (Nursing), Lisa Pinder (Nursing), Dr. Eileen Fitzpatrick (Neuropsychology), as well as MRRI Visiting Scholar, Dr. Lyn Turkstra. Dr. Tessa Hart led an accompanying research study to evaluate the impact of the protocol. The results of this study were recently published in the journal Brain Injury.
Post-traumatic amnesia (PTA) is a state of confusion brought on by physical and chemical changes in the brain after a TBI. Patients may exhibit confusion, disorientation, retrograde amnesia (loss of memory for things that occurred prior to the event), inability to store new memories, and sometimes agitation and delusions. Frequently, patients with TBI are admitted to inpatient rehabilitation during PTA. The duration of PTA may last for a few minutes, or up to several weeks or months depending on the severity of the injury. Hence, many patients with TBI spend a significant portion of their inpatient rehabilitation stay in a state of PTA.
Can patients with memory impairments due to PTA benefit from rehabilitative treatment? Fortunately, the answer appears to be yes. During PTA, the implicit memory system—which enables learning of new skills and routines—is still functioning normally. As a result, rehabilitative approaches that focus on procedural learning are effective. However, difficulties with the explicit memorysystem interfere with learning and recall of fact-based and biographical information. These deficits pose a challenge for communication between patients and their families and care providers.
Patients are asked many questions in the course of treatment that rely on recall of information stored in the explicit memory system—questions about personal history, medical information, orientation, and recent events. Attempts to respond to these questions may cause anxiety and frustration, and furthermore, run the risk of patients providing inaccurate information that may impact the treatment planning process.
The workgroup developed a protocol for identifying patients in PTA, materials to guide communication and treatment, and a staff-training package. The training includes guidance on appropriate treatment and communication strategies, with emphasis on avoiding questions that require retrieval from explicit memory. Instead, clinicians are encouraged to use “here and now questions” and gather clinical information via observation, medical records, or a reliable family member.
Because patients’ rehabilitation experience extends beyond their contact with treating clinicians, separate training materials were developed that were specifically tailored towards staff from ancillary departments—such as dietary, housekeeping, and chaplaincy—who regularly interact with patients in PTA. Educational materials for family members were also provided to help patients’ loved ones understand their communication needs and behaviors. Staff were trained to use informational flyers to educate families on PTA and to guide them in using techniques for communicating with and supporting their loved one during rehabilitation.
Roll-out of the PTA protocol took place at the Drucker Brain Injury Center at MossRehab in 2019. In order to evaluate the impact of the protocol on staff behavior, we observed patients’ interactions with staff during the normal course of an inpatient day both before and after training. We coded the verbal exchanges with attention to inappropriate questions—those that rely on retrieval of information from long-term memory—that were posed to patients in PTA. These inappropriate questions included requests for information from recent or remote memory (e.g. “Do you have any allergies”), or “quiz” type questions where the questioner knows the answer they are looking for (e.g. “What’s my name?”).
Our findings were striking. We saw a significant decrease in the number of information request and quiz-type questions posed to patients, which reduced from over 16 such questions per hour for the typical patient, to fewer than 2. However, the number of appropriate “here and now” questions posed to patients by staff remained unchanged. We also obtained feedback from clinicians in an anonymous survey. The majority reported positive changes in their practice and improved team communication as a result of the training. Clinicians indicated that they were not only reducing the number of declarative memory questions they asked, but they were also providing patients with more information and reassurance.
Recently, Sharon M. Antonucci, PhD, CCC-SLP, was interviewed on the Aphasia Access Conversations podcast. Aphasia is a language impairment that may occur after stroke or other brain injury that can impact a person’s language abilities. Dr. Antonucci is Director of the MossRehab Aphasia Center and a well-known expert on aphasia and aphasia rehabilitation.
In her interview, Dr. Antonucci discusses her work on training semantic feature analysis in conversation groups for people with aphasia and other strategies for aphasia rehabilitation. In particular, she describes her pilot program engaging people in animal-assisted therapy through training dogs. This approach exemplifies the Life Participation Approach to aphasia rehabilitation by helping people with aphasia successfully engage in meaningful interactions and develop new skills that are important to them .
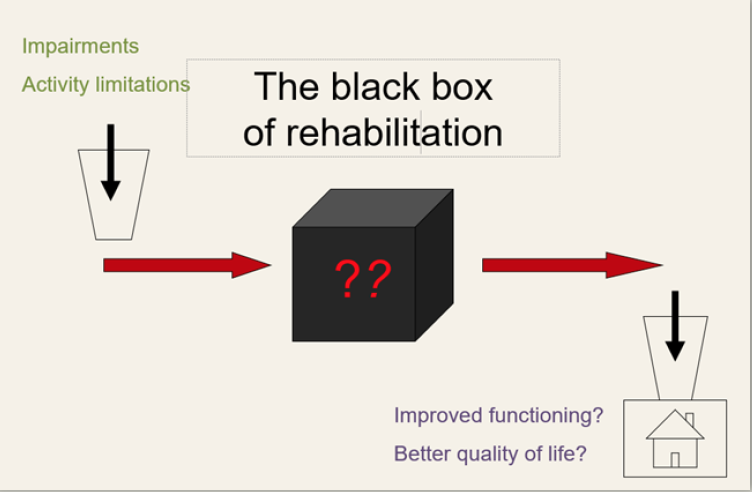
Rehabilitation has been described as a “black box”. We can specify and measure a number of patient features at the time of rehabilitation treatment that predict functional improvement (e.g., demographics, measures of severity). We can also specify and measure the outcomes that rehabilitation treatments hope to achieve. However, we have no shared language for specifying and measuring the rehabilitation treatments themselves. In the case of drug treatments, this is straightforward: specifying the treatment amounts to naming the active chemical ingredient and the dose. In contrast, most rehabilitation treatments involve some form of interaction between clinician and patient/client. What “active ingredients” are delivered during these interactions and in what “dose”?
Until now, we have had only very crude ways of defining rehabilitation treatments. Sometimes we talk about exposure to a particular kind of facility (12 days of inpatient rehabilitation) or discipline (3 one-hour sessions of PT per week). In some cases, we name treatments by the problem they address (gait training, memory remediation). Neither of these approaches is sufficient. Two clinicians providing “gait training” might be pursuing very different training regimens, and we cannot assume that either everything or nothing a PT does in a session is “effective”; we need to know what they did. The current state of rehabilitation treatment specification makes it hard to:
replicate treatment research (replication means delivering the same active ingredients in a new study)
disseminate effective treatments or ensure clinicians are delivering them correctly (i.e. what would a supervisor look for to ensure that the active ingredients are being delivered?)
synthesize evidence across studies (i.e. should we combine studies of memory notebooks, mnemonic strategies, and reminder technology in a meta-analysis because they are all “memory remediation”?)
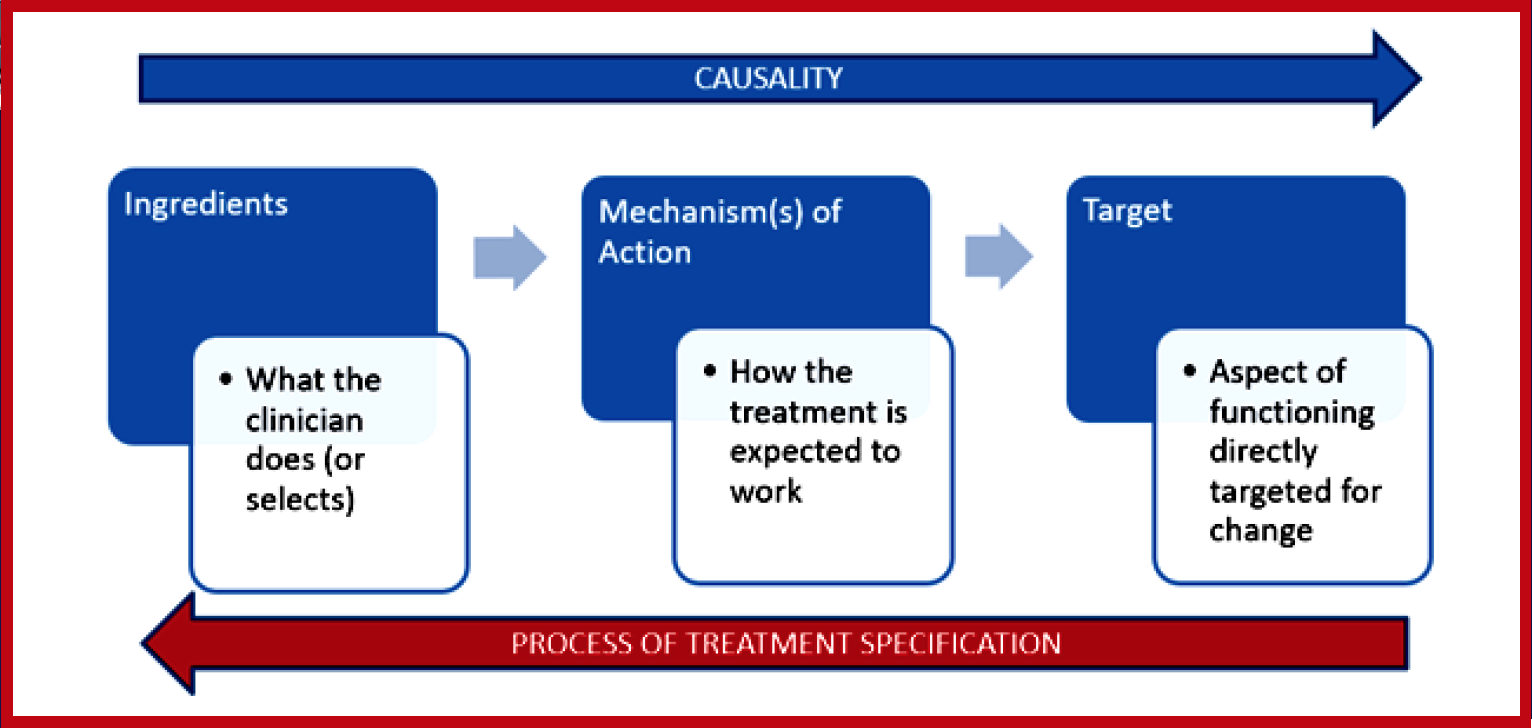
For more than 10 years, a group of rehabilitation scientists and clinicians, at MRRI and elsewhere, have been working to develop a standardized system for specifying any and all rehabilitation treatments. We have established already that there is more than one way to do this, so the question is, Of the many ways that we could define and categorize rehabilitation treatments, which would be most useful in advancing science and practice? We argue for a treatment specification system based on the treatment’s known or hypothesized active ingredients. In this way, testing the efficacy of a treatment called “Treatment X”, is a test of the efficacy of a replicable set of ingredients as well as a test of the theory that those ingredients should produce clinical change: the treatment theory.
With an initial grant from NIDILRR (PI: Marcel Dijkers, PhD), the group developed this conceptual framework, the Rehabilitation Treatment Specification System (RTSS). With subsequent PCORI funding (PI: John Whyte, MD, PhD), these concepts were elaborated into a procedural process in the Manual for Rehabilitation Treatment Specification and described in a set of interrelated articles. The RTSS and its manual have now found a home at the American Congress of Rehabilitation Medicine (ACRM)’s Rehabilitation Treatment Specification Networking Group (RTS-NG), which serves as an organizing hub for the many clinicians and researchers around the world that seek to implement the RTSS framework into their work.
Anticipated benefits of the RTSS have been framed around three areas of rehabilitation: research, clinical practice, and education. We believe that use of the RTSS in the design, replication, and reporting of research will improve the development of treatments. It will encourage more systematic descriptions of the target of the proposed intervention – the direct, functional change that it is designed to cause; as well as the treatment ingredients – what is required in enacting the treatment in order to bring about the desired change in the target. Implementation of research into practice will also benefit, as providing more explicit descriptions of treatments and having a clearer understanding of the relevant components will assist the clinician in using these treatments with their individual patients.
Within clinical practice, use of the RTSS is also expected to enhance clinical reasoning, as the system facilitates consideration of the theoretical mechanisms that underlie rehabilitation treatments. The RTSS recognizes that, for example, many treatments across diverse rehabilitation settings rely on the mechanism that when a skill is practiced in the right way, that skill is improved upon. Whether the skill involved is reaching, articulating a word, or the act of walking, the RTSS directs considerations such as:
What are the important ingredients involved in the practice of that skill?
In what way is that skill desired to be changed?
Is it conceptually plausible? that the ingredients used will make the desired change?
What is the scope of the desired change in terms of generalizability, and will the ingredients support that?
The RTSS also has benefits in clinical education and training. Communication of treatments, both within and across disciplines, is enhanced through not only better identification of these essential elements of treatments as mentioned above, but also by providing a common language and systematic framework to describe treatments.
The RTSS has been used at MossRehab by groups of clinicians, including residents and fellows in MossRehab’s advanced training programs for occupational and physical therapists. While many trainees endorsed the benefits of more thoughtful consideration of both ingredients and targets of treatments, they also encountered some challenges in adopting this new system.
One common issue among clinicians was difficulty learning new RTSS terminology and needing time to “convert” daily documentation to align with RTSS guidelines. Not surprisingly, the extra time is a considerable barrier to clinical implementation. However, over time, we think that barrier will be reduced because academicians are interested in using the RTSS to teach methods of therapy delivery to their students. This conceptual framework can help students link clinical theory to specific actions (ingredients) by facilitating discussion regarding the treatment targets and details of intervention delivery. Active learning experiences during case studies and client simulations can engender habits of clearly describing treatments and evaluating the fit between ingredients and targets. The RTSS provides the structure and terminology to depict how the ingredients can be modified, based on patient performance. As such, students fortified with the RTSS will be better equipped to examine and understand the process of therapeutic change. Further, on a larger scale, colleges with allied health programs now have a structure that crosses multiple disciplines and can naturally enhance their inter-disciplinary education experiences.
These ongoing efforts in education, clinical practice, and research support our hope that the RTSS can be unifying for the field of rehabilitation.
For more information, please see these additional articles on the RTSS:
Amanda Rabinowitz, PhD, was recently selected to be featured in an episode of the People Behind the Science podcast hosted by Marie McNeely PhD. In this interview, Dr. Rabinowitz discusses her exciting ongoing research identifying personal characteristics associated with better recovery trajectories in people following traumatic brain injury (TBI), and how she is applying mobile health technology to help patients better engage in and adhere to rehabilitation. She also speaks about her career path, advice for aspiring scientists, and the excellent mentors who helped cultivate and refine her research interests. Dr. Rabinowitz also gives listeners insight into her passions outside of research, including her love of cooking and baking sourdough bread.
Dr. Rabinowitz is an institute scientist and director of the Brain Injury Neuropsychology Laboratory, which examines the neurobiological and psychosocial factors that influence recovery from TBI across the spectrum of injury severity.
Amanda Therrien, PhD New Grant Award and Paper Accepted
Amanda Rabinowitz, PhD Paper Published
Tessa Hart, PhD Paper Published
Dylan Edwards, PhD New Book Chapter Published
Moss Rehabilitation Research Institute scientists and staff members had a variety of accomplishments and events to celebrate during the month of August. First, we would like to congratulate Laurel Buxbaum, PsyD, and Amanda Therrien, PhD, who each received new grant awards from the Peer Review Committee (PRC). Under her award, Dr. Buxbaum will conduct initial feasibility and pilot studies using virtual reality to assess arm choice under cognitive load in people after stroke. Dr. Therrien’s award will fund a pilot study to assess behavioral predictors of responsiveness to a new movement training intervention for cerebellar ataxia.
Last month, we were also pleased to welcome two new postdoctoral scholars to our team of exceptional researchers. They have been meeting remotely with their mentors and have begun work on research activities. You can learn more about MRRI postdocs Haley Dresang, PhD, and Cory Potts, PhD, in our recent blog article. We also published a new blog post on the Parkinson’s Extension of the MRRI Research Registry featuring Emily Fannick and Katie Cornell, key staff members involved in recruiting new research volunteers.
MRRI scientists continued to make important contributions to the scientific literature in the field of neurorehabilitation with five new publications that were published or accepted for publication in peer-reviewed journals.
One of these papers, authored by Tessa Hart, PhD, Amanda Rabinowitz, PhD, and collaborators, describes the development and impact of a clinical protocol to improve communication with patients experiencing post-traumatic amnesia following brain injury. Post-traumatic amnesia commonly occurs immediately following a traumatic brain injury (TBI) and is characterized by confusion, disorientation, and memory loss. This protocol was developed to help clinicians better treat and effectively communicate with patients with TBI.
Amanda Therrien, PhD, and collaborators also published an article which builds upon their previous work studying a new method of movement training for individuals with cerebellar ataxia – a condition is normally associated with impaired motor learning. By altering training conditions to leverage reinforcement-based learning mechanisms that do not depend on the cerebellum, they showed that individuals with cerebellar ataxia can learn, in a complex reaching task, to reduce features of their ataxia. This work suggests that reinforcement-based interventions may hold promise as a new method to improve rehabilitation training for cerebellar ataxia.
In addition, Dylan Edwards, PhD, was selected among top experts to co-author a chapter in a new edition of the book Neurovascular Neuropsychology. This book provides updated information on our understanding of the brain and its blood supply, including advances in medical and surgical treatments and their impacts on neurocognitive outcomes. The chapter to which he contributed describes the state of the evidence and new advances in application of non-invasive brain stimulation to facilitate recovery in stroke survivors.
We are pleased to acknowledge these recent successes, and our scientists look forward to continuing to make important contributions to the field of neurorehabilitation research to improve the lives of individuals with neurological disabilities.